

Lupus in the Caribbean: The hidden burden, the missing data and the new fight to change outcomes
.jpg)
In the Caribbean, lupus remains one of the region’s quieter health threats: under-discussed, unevenly tracked, often misunderstood and potentially devastating when diagnosed late. It is not a rare inconvenience. It is a chronic autoimmune disease in which the immune system turns against the body itself, attacking healthy tissue and causing inflammation that can damage the skin, joints, kidneys, blood cells, brain, heart and lungs. For many patients, it arrives in waves, with periods of illness and periods of remission, but the danger is that even when symptoms seem manageable, organ damage can be quietly advancing.
The Caribbean has particular reason to pay attention. Lupus is known to affect women far more often than men, usually during the years when they are building families, careers and lives. Global data show that about 90 percent of people living with lupus are women, with most developing the disease between ages 15 and 44. The Lupus Foundation of America estimates at least five million people worldwide have a form of lupus, and systemic lupus accounts for about 70 percent of all lupus cases.
For Caribbean populations, the concern is sharper because people of African ancestry and mixed ancestry are disproportionately affected, often with more serious organ involvement. The U.S. National Institute of Arthritis and Musculoskeletal and Skin Diseases notes that lupus is more common among African Americans than White people, and that men, African Americans, Chinese people and Hispanic people are more likely to have serious organ system involvement.
The Caribbean numbers tell a serious story
The difficulty in writing about lupus in the Caribbean is also part of the story: many territories do not have comprehensive, updated lupus registries. That means the region is still relying heavily on studies from Barbados, Puerto Rico, Curaçao, Martinique and St. Lucia, along with wider research on African-Caribbean populations.
Still, the available figures are striking.
In Barbados, one of the most important lupus studies in the English-speaking Caribbean found that between 2000 and 2009, the incidence of systemic lupus erythematosus was 12.21 per 100,000 person-years among women, compared to 0.84 per 100,000 among men. The same research showed how serious the disease becomes when kidneys are involved: Barbados reported an overall five-year survival rate of 79.9 percent, but survival fell to 68 percent among patients with lupus nephritis.
That kidney burden matters because lupus nephritis, kidney disease caused by lupus, is one of the most dangerous complications. In the Barbados data, nephritis affected nearly half of patients. A separate summary of the Barbados registry reported that the main presenting manifestations included arthritis at 84 percent, nephritis at 47 percent, pleuritis at 41.5 percent, malar rash at 36.4 percent and discoid lesions at 33.1 percent.
Other Caribbean figures add to the concern. Research cited in a 2024 review of lupus across the African diaspora reported estimated lupus incidence of 8.0 per 100,000 person-years in St. Lucia and 4.7 per 100,000 person-years in Martinique. The same review noted that survival varied considerably across territories, with Martinique, supported by specialized lupus centers and socialized healthcare, showing 10-, 15- and 20-year survival rates of 95.5 percent, 94.4 percent and 92.1 percent, respectively. St. Lucia, where patient education and empowerment were emphasized in a private rheumatology setting, reported five-year survival of 97 percent among non-impoverished participants.
Puerto Rico also stands out. A 2007 study estimated overall lupus prevalence at 159 per 100,000 people, with prevalence far higher among women, 277 per 100,000, compared to 25 per 100,000 among men.
Curaçao’s older but still important data showed an average annual incidence rate of 4.6 per 100,000, annual mortality of 1.7 per 100,000 and renal disease in 78 percent of patients. The study concluded that environmental factors may play a major role in disease expression among Black populations in Curaçao.
Taken together, these figures point to a Caribbean lupus reality that is both medical and social. The disease is not only appearing in the region, it is appearing in populations already challenged by specialist shortages, uneven access to diagnostic tests, high out-of-pocket costs, fragmented data and limited public awareness.
The disease of many faces
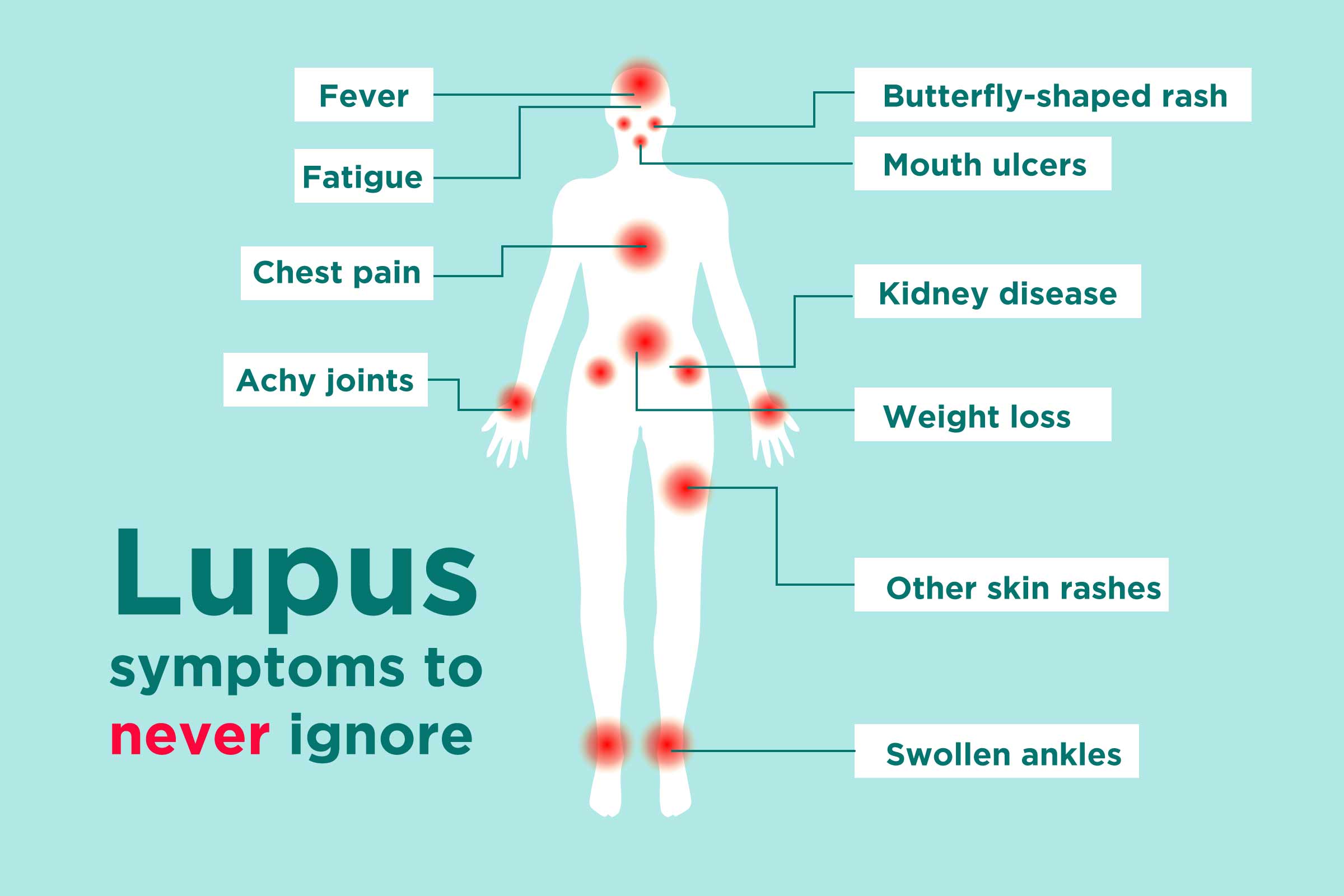
Lupus is often called difficult to diagnose because it does not behave the same way in every patient. Symptoms can include swollen and painful joints, unexplained fever, fatigue, rashes, sun sensitivity, hair loss, mouth sores, chest pain, neurological symptoms and swelling around the eyes or legs. Some patients look healthy while dealing with pain, exhaustion and internal inflammation. Others are not diagnosed until the disease has already attacked the kidneys or other organs.
In the Caribbean, where sun exposure is part of everyday life and where many people delay care because of cost, stigma or lack of access, early symptoms can be brushed aside. Fatigue becomes “stress.” Joint pain becomes “getting older.” Skin rashes may be treated cosmetically rather than medically. Swelling may not trigger urgent kidney screening. By the time the patient reaches a specialist, the disease may have already moved from discomfort to damage.
The public awareness gap is global, but it has Caribbean implications. A 2026 World Lupus Federation survey found that 58 percent of respondents worldwide knew little or nothing about lupus. Even among people familiar with lupus, 48 percent did not know or were unsure that it can affect any organ, 46 percent were unaware it can be fatal and 41 percent did not know or were unsure that symptoms vary widely from person to person.
That lack of knowledge can delay diagnosis. It can also deepen stigma. The same survey found that 19 percent of respondents believed lupus was contagious, while 21 percent said they would be uncomfortable sharing food with someone with lupus and 18 percent said they would hesitate to hug someone with the disease.
For small island communities, where privacy is limited and misinformation travels quickly, that stigma can discourage people from speaking openly, seeking support or disclosing their condition at work.
The kidney crisis inside the lupus crisis
The most urgent issue in the fight against lupus is kidney disease. Lupus nephritis can lead to kidney failure, dialysis or transplant. It can also be missed in its early stages because symptoms may be subtle or absent.
A 2025 World Lupus Federation global survey of more than 3,260 people with lupus from 84 countries found that 47 percent reported kidney involvement. More than 43 percent said they had little or no knowledge about lupus nephritis, even though 85 percent reported one or more symptoms associated with it. Among those diagnosed with lupus nephritis, 59 percent reported being hospitalized because of it.
The same survey found that more than one third of respondents reporting a lupus nephritis diagnosis had not had a kidney biopsy, which is considered the gold standard for diagnosis, while 54 percent of those who had not had a biopsy said they were hesitant to undergo the procedure.
This matters for the Caribbean because the region’s lupus burden is closely tied to kidney involvement. Barbados and Curaçao data both point to high rates of renal disease, and the difference in survival between patients with and without nephritis shows why early urine testing, blood pressure checks, creatinine monitoring and specialist referral should be treated as basic lupus care, not advanced care.
New treatments are changing the fight
The fight against lupus is entering a new phase. For decades, many patients depended heavily on steroids and broad immunosuppressive drugs. These medicines can control inflammation, but long-term steroid use carries serious risks, including infection, diabetes, bone damage, weight gain, high blood pressure and cardiovascular complications.
Newer therapies are more targeted. Belimumab, sold as Benlysta, became the first biologic approved for systemic lupus and later expanded into lupus nephritis treatment. In June 2025, the U.S. Food and Drug Administration approved a 200 mg/mL Benlysta autoinjector for children five years and older with active lupus nephritis, allowing at-home subcutaneous treatment for eligible pediatric patients receiving standard therapy. GSK noted that lupus nephritis develops in about 30 to 50 percent of children with lupus, often within one to two years of diagnosis.
Another important development is anifrolumab, sold as Saphnelo. The intravenous form was approved in 2021 for adults with moderate to severe systemic lupus erythematosus receiving standard therapy. In April 2026, U.S. regulators approved a once-weekly self-administered autoinjector version for adults with systemic lupus erythematosus, based on Phase III TULIP-SC trial results showing reduced disease activity compared with placebo while patients continued standard therapy.
For Caribbean patients, the importance of at-home options cannot be overstated. In many territories, a patient may have to miss work, pay transportation costs or travel between islands to access specialist care. An approved self-injection option does not solve the affordability problem, but it can reduce the burden of repeated clinic visits where the medicine is available and covered.
Voclosporin, sold as Lupkynis, is another major treatment in lupus nephritis. It was approved as the first oral treatment specifically for adults with active lupus nephritis in combination with standard care.
These developments represent progress, but access remains the central Caribbean question. A medicine approved in the United States or Europe is not automatically affordable, stocked, reimbursed or prescribed in small island health systems. The science is advancing faster than many local systems can absorb.
The next frontier: resetting the immune system
Beyond current medications, researchers are now exploring approaches that could reshape lupus treatment altogether. One of the most watched areas is CAR T-cell therapy, originally developed for certain blood cancers. In autoimmune disease, the idea is to reprogram immune cells to target rogue B cells involved in the autoimmune attack.
The Associated Press reported in 2025 that scientists are testing approaches aimed at reprogramming dysfunctional immune systems rather than only suppressing them. CAR T-cell trials are being explored in lupus and other autoimmune diseases, with early cases showing some patients reaching remission after exhausting standard treatments. Researchers are also studying regulatory T cells, T-cell engagers and mRNA-based methods that could one day help retrain immune responses more precisely.
The Lupus Research Alliance also highlighted the growing importance of advanced biomarkers, genetic profiling, predictive analytics, engineered cell therapy and patient-centered care in the evolving lupus research landscape.
For the Caribbean, this frontier is both hopeful and distant. CAR T-cell therapy is expensive, complex and still largely experimental for lupus. It requires advanced centers, trained teams, careful monitoring and systems capable of managing serious side effects. But it also points to where the global fight is heading: earlier detection, better risk prediction, more personalized treatment and less dependence on long-term steroid exposure.

The Caribbean gap: data, diagnosis and access
The region’s biggest lupus challenge may not be a lack of knowledge somewhere in the world. It is the uneven translation of that knowledge into Caribbean systems.
Too many islands lack updated population-level lupus data. Without registries, governments cannot accurately estimate how many people are living with lupus, how many have kidney disease, how often patients are hospitalized, how long diagnosis takes, what medicines are being used and how many patients are losing income or quality of life because of the disease.
The Caribbean also needs stronger pathways for diagnosis. That means primary care doctors must be trained to suspect lupus earlier, particularly in young women with unexplained fatigue, joint pain, rashes, swelling, abnormal urine tests or recurrent fevers. It means laboratories must be able to process relevant autoimmune tests consistently. It means kidney screening must become routine for diagnosed patients. It also means rheumatology, nephrology and mental health support must be connected, because lupus is not only a physical disease, it affects work, family life, fertility decisions, emotional health and financial stability.
The region’s small size can actually become an advantage. Caribbean territories can build shared registries, use tele-rheumatology, pool procurement for high-cost medications, develop common treatment protocols and run public education campaigns across multiple islands. PAHO’s broader 2026 focus on strengthening clinical trials in the Americas through tools such as the Portal of Clinical Trials of the Americas also points to a larger regional opportunity: Caribbean patients should not be invisible in research that will shape future care.
What the fight should look like now
The next phase of lupus care in the Caribbean should begin with recognition. Lupus is not simply “aches and pains.” It is not contagious. It is not only a women’s issue, although women carry most of the burden. It is not always visible, and it is not always mild.
A serious Caribbean response would include national or regional lupus registries, routine kidney screening for every lupus patient, public education campaigns, specialist referral protocols, training for general practitioners, improved access to biologics and newer lupus nephritis therapies, and stronger support for patients who struggle with employment, insurance, fertility planning and long-term disability.
The figures already available make the case. Barbados shows high incidence among women and sharply worse survival when kidneys are involved. Curaçao shows high renal complication rates. Puerto Rico shows high prevalence. Global surveys show deep gaps in public knowledge and kidney awareness. New treatments show that better outcomes are possible, but only if health systems are organized enough to deliver them.
For the Caribbean, the fight against lupus is now a fight on two fronts. One is scientific, where new therapies are changing what doctors can offer. The other is structural, where governments, health insurers, clinicians and patient groups must ensure that Caribbean patients are not left waiting for yesterday’s care while tomorrow’s medicine moves ahead without them.